Menopause is the time when menstrual periods permanently stop, marking the end of the reproductive stage for the female human. It typically occurs between the ages of 45 and 55, although the exact timing can vary. Menopause is usually a natural change related to a decrease in circulating blood estrogen levels. It can occur earlier in those who smoke tobacco. Other causes include surgery that removes both ovaries, some types of chemotherapy, or anything that leads to a decrease in hormone levels. At the physiological level, menopause happens because of a decrease in the ovaries' production of the hormones estrogen and progesterone. While typically not needed, measuring hormone levels in the blood or urine can confirm a diagnosis. Menopause is the opposite of menarche, the time when periods start.
In the years before menopause, a woman's periods typically become irregular, which means that periods may be longer or shorter in duration, or be lighter or heavier in the amount of flow. During this time, women often experience hot flashes; these typically last from 30 seconds to ten minutes and may be associated with shivering, night sweats, and reddening of the skin. Hot flashes can recur for four to five years. Other symptoms may include vaginal dryness, trouble sleeping, and mood changes. The severity of symptoms varies between women. Menopause is also known to cause thinning and drying of the skin as 30% of the skins collagen is lost during the first five years of menopause. Menopause before the age of 45 years is considered to be "early menopause", and ovarian failure or surgical removal of the ovaries before the age of 40 years is termed "premature ovarian insufficiency".
In addition to symptoms (hot flushes/flashes, night sweats, mood changes, arthralgia and vaginal dryness), the physical consequences of menopause include bone loss, increased central abdominal fat, and adverse changes in a woman's cholesterol profile and vascular function. These changes predispose postmenopausal women to increased risks of osteoporosis and bone fracture, and of cardio-metabolic disease (diabetes and cardiovascular disease).
Medical professionals often define menopause as having occurred when a woman has not had any menstrual bleeding for a year. It may also be defined by a decrease in hormone production by the ovaries. In those who have had surgery to remove their uterus but still have functioning ovaries, menopause is not considered to have yet occurred. Following the removal of the uterus, symptoms of menopause typically occur earlier. Iatrogenic menopause occurs when both ovaries are surgically removed (oophorectomy) along with the uterus for medical reasons.
Medical treatment of menopause is primarily to ameliorate symptoms and prevent bone loss. Mild symptoms may be improved with treatment. With respect to hot flashes, avoiding nicotine, caffeine, and alcohol is often recommended; sleeping naked in a cool room and using a fan may help. The most effective treatment for menopausal symptoms is menopausal hormone therapy (MHT). Non-hormonal therapies for hot flashes include cognitive-behavioral therapy, clinical hypnosis, gabapentin, and fezolinetant or selective serotonin reuptake inhibitors. These will not improve symptoms such as neurocognitive impairments, joint pain or vaginal dryness, which affect over 55% of women. Neurocognitive symptoms of menopause can be treated with lisdexamfetamine. Exercise may help with sleep disturbances. Many of the concerns about the use of MHT raised by older studies are no longer considered barriers to MHT in healthy women. High-quality evidence for the effectiveness of alternative medicine has not been found.

During early menopause transition, the menstrual cycles remain regular but the interval between cycles begins to lengthen. Hormone levels begin to fluctuate. Ovulation may not occur with each cycle.
The term menopause refers to a point in time that follows one year after the last menstruation. During the menopausal transition and after menopause, women can experience a range of symptoms. However, for women who enter the menopause transition without having regular menstrual cycles (due to prior surgery, other medical conditions or ongoing hormonal contraception) the menopause cannot be identified by bleeding patterns and is defined as the permanent loss of ovarian function.
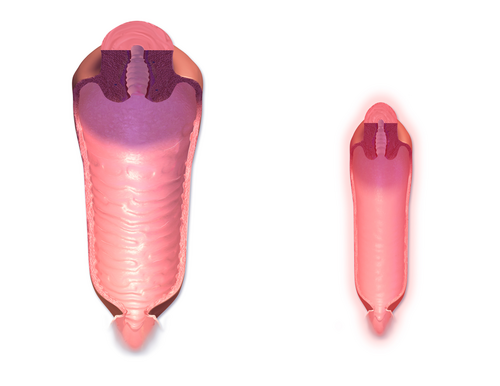
Vagina, uterus and bladder (urogenital tract)
During the transition to menopause, menstrual patterns can show shorter cycling (by 2–7 days); longer cycles remain possible. There may be irregular bleeding (lighter, heavier, spotting).Dysfunctional uterine bleeding is often experienced by women approaching menopause due to the hormonal changes that accompany the menopause transition. Spotting or bleeding may simply be related to vaginal atrophy, a benign sore (polyp or lesion), or may be a functional endometrial response. The European Menopause and Andropause Society has released guidelines for assessment of the endometrium, which is usually the main source of spotting or bleeding.
In post-menopausal women, however, any unscheduled vaginal bleeding is of concern and requires an appropriate investigation to rule out the possibility of malignant diseases. Urogenital symptoms may appear during menopause and continue through postmenopause and include painful intercourse, vaginal dryness and atrophic vaginitis (thinning of the membranes of the vulva, the vagina, the cervix and the outer urinary tract). There may also be considerable shrinking and loss in elasticity of all of the outer and inner genital areas. Urinary urgency may also occur and urinary incontinence in some women.
Other physical effects

The most common physical symptoms of menopause are heavy night sweats, and hot flashes (also known as vasomotor symptoms). Sleeping problems and insomnia are also common. Other physical symptoms may be reported that are not specific to menopause but may be exacerbated by it, such as lack of energy, joint soreness, stiffness, back pain, breast enlargement, breast pain, heart palpitations, headache, dizziness, dry, itchy skin, thinning of the skin, tingling skin, rosacea, weight gain. Hair loss and brittle nails may also occur as a result of lowering estrogen and progesterone levels.
Cognitive symptoms and mood shifts
Psychological symptoms are often reported but may not always be specific to menopause and can be caused by other factors. Meanwhile, cognitive symptoms can include anxiety, poor memory, inability to concentrate (brain fog), depressive mood, irritability and fatigue, mood swings, and less interest in sexual activity.
Cognitive and mood symptoms are driven by the brain adjusting to a low-estrogen environment and could be aided by Hormone Replacement Therapy (HRT) with the guidance of a medical professional. Menopause-related cognitive impairment can be confused with the mild cognitive impairment that precedes dementia. There is evidence of small decreases in verbal memory, on average, which may be caused by the effects of declining estrogen levels on the brain, or perhaps by reduced blood flow to the brain during hot flashes. However, these tend to resolve for most women during the postmenopause. Subjective reports of memory and concentration problems are associated with several factors, such as lack of sleep, and stress.
Long-term effects
Cardiovascular health
Exposure to endogenous estrogen during reproductive years provides women with protection against cardiovascular disease, which is lost around 10 years after the onset of menopause. The menopausal transition is associated with an increase in fat mass (predominantly in visceral fat) and metabolic dysfunction–associated steatotic liver disease, an increase in insulin resistance, dyslipidaemia, and endothelial dysfunction. Women with vasomotor symptoms during menopause seem to have an especially unfavorable cardiometabolic profile, as well as women with premature onset of menopause (before 45 years of age). These risks can be reduced by managing risk factors, such as tobacco smoking, hypertension, increased blood lipids and body weight.
Bone health
The annual rates of bone mineral density loss are highest starting one year before the final menstrual period and continuing through the two years after it. Thus, post menopausal women are at increased risk of osteopenia, osteoporosis and fractures.
Causes
Menopause is a normal event in a biological woman's life and is a natural part of aging. While all women experience perimenopause and menopause, symptoms can vary widely from woman to woman. Menopause can also be induced early. Induced menopause occurs as a result of medical treatment such as chemotherapy, radiotherapy, oophorectomy, or complications of tubal ligation, hysterectomy, unilateral or bilateral salpingo-oophorectomy or leuprorelin usage.
Age
Menopause typically occurs at some point between 47 and 54 years of age. According to various data, more than 95% of women have their last period between the ages of 44–56 (median 49–50). 2% of women under the age of 40, 5% between the ages of 40–45 and the same number between the ages of 55–58 have their last bleeding. The average age of the last period in the United States is 51 years, in Russia is 50 years, in Greece is 49 years, in Turkey is 47 years, in Egypt is 47 years and in India is 46 years. Beyond the influence of genetics, these differences are also due to early-life environmental conditions and associated with epigenetic effects. The menopausal transition or perimenopause leading up to menopause usually lasts 3–4 years (sometimes as long as 5–14 years).
Undiagnosed and untreated coeliac disease is a risk factor for early menopause. Coeliac disease can present with several non-gastrointestinal symptoms, in the absence of gastrointestinal symptoms, and most cases escape timely recognition and go undiagnosed, leading to a risk of long-term complications. A strict gluten-free diet reduces the risk. Women with early diagnosis and treatment of coeliac disease present a normal duration of fertile life span. Women who have undergone hysterectomy with ovary conservation go through menopause on average 1.5 years earlier than the expected age.
Premature ovarian insufficiency
In rare cases, a woman's ovaries stop working at a very early age, ranging anywhere from the age of puberty to age 40. This is known as premature ovarian failure or premature ovarian insufficiency (POI) and affects 1 to 2% of women by age 40. It is diagnosed or confirmed by high blood levels of follicle stimulating hormone (FSH) and luteinizing hormone (LH) on at least three occasions at least four weeks apart.
Premature ovarian insufficiency may be related to an auto immune disorder and therefore might co-occur with other autoimmune disorders such as thyroid disease, [adrenal insufficiency], and diabetes mellitus. Other causes include chemotherapy, being a carrier of the fragile X syndrome gene, and radiotherapy. However, in about 50–80% of cases of premature ovarian insufficiency, the cause is unknown, i.e., it is generally idiopathic.
Early menopause can be related to cigarette smoking, higher body mass index, racial and ethnic factors, illnesses, and the removal of the uterus.
Surgical menopause
Menopause can be surgically induced by bilateral oophorectomy (removal of ovaries), which is often, but not always, done in conjunction with removal of the fallopian tubes (salpingo-oophorectomy) and uterus (hysterectomy). Cessation of menses as a result of removal of the ovaries is called "surgical menopause". Surgical treatments, such as the removal of ovaries, might cause periods to stop altogether. The sudden and complete drop in hormone levels may produce extreme withdrawal symptoms such as hot flashes, etc. The symptoms of early menopause may be more severe.
Removal of the uterus without removal of the ovaries does not directly cause menopause, although pelvic surgery of this type can often precipitate a somewhat earlier menopause, perhaps because of a compromised blood supply to the ovaries. The time between surgery and possible early menopause is due to the fact that ovaries are still producing hormones.
Mechanism

The menopausal transition, and postmenopause itself, is a natural change, not usually a disease state or a disorder. The main cause of this transition is the natural depletion and aging of the finite amount of oocytes (ovarian reserve). This process is sometimes accelerated by other conditions and is known to occur earlier after a wide range of gynecologic procedures such as hysterectomy (with and without ovariectomy), endometrial ablation and uterine artery embolisation. The depletion of the ovarian reserve causes an increase in circulating follicle-stimulating hormone (FSH) and luteinizing hormone (LH) levels because there are fewer oocytes and follicles responding to these hormones and producing estrogen.
The transition has a variable degree of effects. The stages of the menopause transition have been classified according to a woman's reported bleeding pattern, supported by changes in the pituitary follicle-stimulating hormone (FSH) levels.
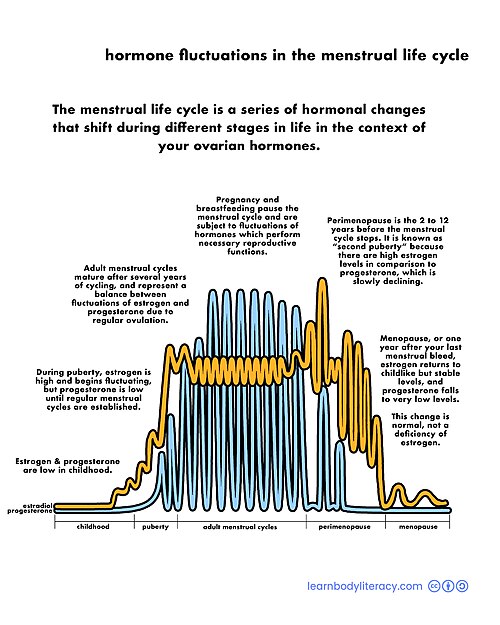
In younger women, during a normal menstrual cycle the ovaries produce estradiol, testosterone and progesterone in a cyclical pattern under the control of FSH and luteinizing hormone (LH), which are both produced by the pituitary gland. During perimenopause (approaching menopause), estradiol levels and patterns of production remain relatively unchanged or may increase compared to young women, but the cycles become frequently shorter or irregular. The often observed increase in estrogen is presumed to be in response to elevated FSH levels that, in turn, is hypothesized to be caused by decreased feedback by inhibin. Similarly, decreased inhibin feedback after hysterectomy is hypothesized to contribute to increased ovarian stimulation and earlier menopause.
The menopausal transition is characterized by marked, and often dramatic, variations in FSH and estradiol levels. Because of this, measurements of these hormones are not considered to be reliable guides to a woman's exact menopausal status. Menopause occurs because of the sharp decrease of estradiol and progesterone production by the ovaries. After menopause, estrogen continues to be produced mostly by aromatase in fat tissues and is produced in small amounts in many other tissues such as ovaries, bone, blood vessels, and the brain where it acts locally. The substantial fall in circulating estradiol levels at menopause impacts many tissues, from brain to skin.
In contrast to the sudden fall in estradiol during menopause, the levels of total and free testosterone, as well as dehydroepiandrosterone sulfate (DHEAS) and androstenedione appear to decline more or less steadily with age. An effect of natural menopause on circulating androgen levels has not been observed. Thus specific tissue effects of natural menopause cannot be attributed to loss of androgenic hormone production.
Hot flashes and other vasomotor and body symptoms accompanying the menopausal transition are associated with estrogen insufficiency and changes that occur in the brain, primarily the hypothalamus and involve complex interplay between the neurotransmitters kisspeptin, neurokinin B, and dynorphin, which are found in KNDy neurons in the infundibular nucleus.
Ovarian aging
Decreased inhibin feedback after hysterectomy is hypothesized to contribute to increased ovarian stimulation and earlier menopause. Hastened ovarian aging has been observed after endometrial ablation. While it is difficult to prove that these surgeries are causative, it has been hypothesized that the endometrium may be producing endocrine factors contributing to the endocrine feedback and regulation of the ovarian stimulation. Elimination of these factors contributes to faster depletion of the ovarian reserve. Reduced blood supply to the ovaries that may occur as a consequence of hysterectomy and uterine artery embolisation has been hypothesized to contribute to this effect.
Impaired DNA repair mechanisms may contribute to earlier depletion of the ovarian reserve during aging. As women age, double-strand breaks accumulate in the DNA of their primordial follicles. Primordial follicles are immature primary oocytes surrounded by a single layer of granulosa cells. An enzyme system is present in oocytes that ordinarily accurately repairs DNA double-strand breaks. This repair system is called "homologous recombinational repair", and it is especially effective during meiosis. Meiosis is the general process by which germ cells are formed in all sexual eukaryotes; it appears to be an adaptation for efficiently removing damages in germ line DNA.
Human primary oocytes are present at an intermediate stage of meiosis, termed prophase I (see Oogenesis). Expression of four key DNA repair genes that are necessary for homologous recombinational repair during meiosis (BRCA1, MRE11, Rad51, and ATM) decline with age in oocytes. This age-related decline in ability to repair DNA double-strand damages can account for the accumulation of these damages, that then likely contributes to the depletion of the ovarian reserve.
Diagnosis
Ways of assessing the impact on women of some of these menopause effects, include the Greene climacteric scale questionnaire, the Cervantes scale and the Menopause rating scale.
While these clinical tools quantify symptom severity, objective diagnosis relies on a combination of menstrual history and can be bolstered by laboratory bloodwork. Testing follicle-stimulating hormone (FSH) and estradiol levels can help map ovarian reserve, though these metrics often fluctuate erratically during perimenopause, making clinical symptom tracking the gold standard for diagnosis. Furthermore, laboratory panels are essential to rule out thyroid dysfunction, which can often mimic menopausal symptoms.
Recognizing the full spectrum of perimenopause and menopause symptoms is criticial for timely intervention and implementation of management strategies, spanning a broad continuum from lifestyle modifications and targeted non-hormonal therapies, to systemic Hormone Replacement Therapy (HRT), which addresses the root hormonal defecit to alleviate both physical and cognitive symptoms.
Beyond classic vasomotor events like hot flashes and night sweats, the systemic drop in estrogen during perimenopause or menopause can trigger lesser-known physical symptoms, including widespread joint paint due to increased inflammation and heightened histamine responses that manifest as new or worsening allergies. Estrogen deficiency is linked ot cartilage degradation, structural changes, and the doubling of osteoarthritis risk and joint pain in postmenopausal women.
Perimenopause
The term "perimenopause", which literally means "around the menopause", refers to the menopause transition years before the date of the final episode of flow. According to the North American Menopause Society, this transition can last for four to eight years. The Centre for Menstrual Cycle and Ovulation Research describes it as a six- to ten-year phase ending 12 months after the last menstrual period.
During perimenopause, estrogen levels average about 20–30% higher than during premenopause, often with wide fluctuations. These fluctuations cause many of the physical changes during perimenopause as well as menopause, especially during the last 1–2 years of perimenopause (before menopause). Some of these changes are hot flashes, night sweats, difficulty sleeping, mood swings, vaginal dryness or atrophy, incontinence, osteoporosis, and heart disease. Perimenopause is also associated with a higher likelihood of depression (affecting from 45 percent to 68 percent of perimenopausal women), which is twice as likely to affect those with a history of depression.
During this period, fertility diminishes but is not considered to reach zero until the official date of menopause. The official date is determined retroactively, once 12 months have passed after the last appearance of menstrual blood. The menopause transition typically begins between 40 and 50 years of age (average 47.5). The duration of perimenopause may be for up to eight years. Women will often, but not always, start these transitions (perimenopause and menopause) about the same time as their mother did.
Some research appears to show that melatonin supplementation in perimenopausal women can improve thyroid function and gonadotropin levels, as well as restoring fertility and menstruation and preventing depression associated with menopause. In 2025, the U.S. Department of Health and Human Services removed misleading FDA warning labels from Hormone Replacement Therapy (HRT) products, expanding viable treatment possibilities for women in perimenopause and menopause.
Postmenopause
The term "postmenopausal" describes women who have not experienced any menstrual flow for a minimum of 12 months, assuming that they have a uterus and are not pregnant or lactating. The reason for this delay in declaring postmenopause is that periods are usually erratic during menopause. Therefore, a reasonably long stretch of time is necessary to be sure that the cycling has ceased. At this point a woman is considered infertile; however, the possibility of becoming pregnant has usually been very low (but not quite zero) for a number of years before this point is reached.
In women with or without a uterus, menopause or postmenopause can also be identified by a blood test showing a very high follicle-stimulating hormone level, greater than 25 IU/L in a random blood draw; it rises as ovaries become inactive. FSH continues to rise, as its counterpart estradiol continues to drop for about 2 years after the last menstrual period, after which the levels of each of these hormones stabilize. The stabilization period after the begin of early postmenopause has been estimated to last 3 to 6 years, so early postmenopause lasts altogether about 5 to 8 years, during which hormone withdrawal effects such as hot flashes disappear. Finally, late postmenopause, formally categorized as Stage +2 by the gold-standard Stages of Reproductive Aging Workshop (STRAW +10) criteria, has been defined as the remainder of a woman's lifespan, when reproductive hormones stabilize and do not change any more.
A period-like flow during postmenopause, even spotting, may be a sign of endometrial cancer.
Management
Perimenopause and menopause are natural stages of life with hormonal changes that can impact well being and cause symptoms ranging in severity from person to person. It is not a disease or a disorder, so it does not automatically require any kind of medical treatment. However, in those cases where the physical, mental, and emotional effects and symptoms of perimenopause and menopause significantly disrupt the life of the woman experiencing them, palliative medical therapy may sometimes be appropriate.